Early this week, Gerard Rivera and I joined Xtalks for a live webinar on one of the most pressing — and least visible — challenges in pharma today: gross-to-net (GTN) leakage.
(You can register to view the full recording here. But if you’d like to go deeper in a confidential, custom discussion of your drug brand, join us at Asembia in Las Vegas later this month or reach out to us.)
Here’s what you need to know:
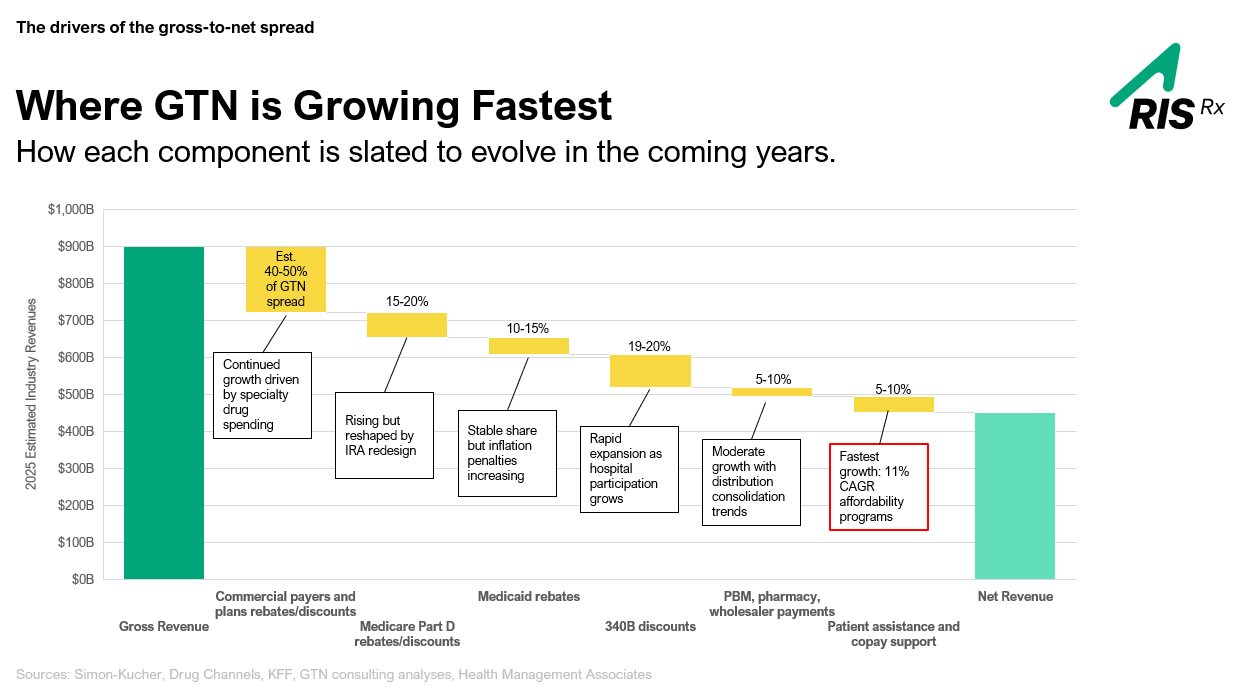
1. The $90 Billion Number Is Real — and It’s Getting Worse
We opened by asking a simple question: where do GTN dollars actually go? And once we mapped the waterfall — from gross list price down through rebates, Medicaid, 340B, and affordability programs — the picture got uncomfortable fast.
Of an estimated $55 billion in copay spend in 2024 alone, approximately 20% leaked out. That’s $11 billion in lost revenue that could have been protected. And when you layer in 340B and commercial rebates, total estimated leakage balloons to nearly $90 billion industrywide. Not a rounding error.
What’s more, affordability programs are now the fastest-growing GTN bucket — at an 11% CAGR. That means every dollar you spend on patient support has more leakage risk attached to it than ever before. The problem isn’t shrinking. It’s compounding.
2. Copay Support Is a Clinical Issue, Not Just a Financial One
One of the points Gerard made that I think lands hardest is this: GTN isn’t just a finance team problem. Every dollar that leaks creates friction for a real patient.
We’re in an environment where deductibles keep rising, accumulators and maximizers now affect more than 80% of commercially insured patients, and pharmacies are under serious reimbursement pressure. The result? Co-pay support has gone from “nice to have” to the lifeline that determines whether a patient stays on therapy at all.
When patients can’t afford their medication, they don’t just delay care. They abandon it entirely. And when that happens, outcomes suffer. The financial and clinical stories are inseparable, which means the people managing GTN and the people managing patient services need to be working from the same playbook.
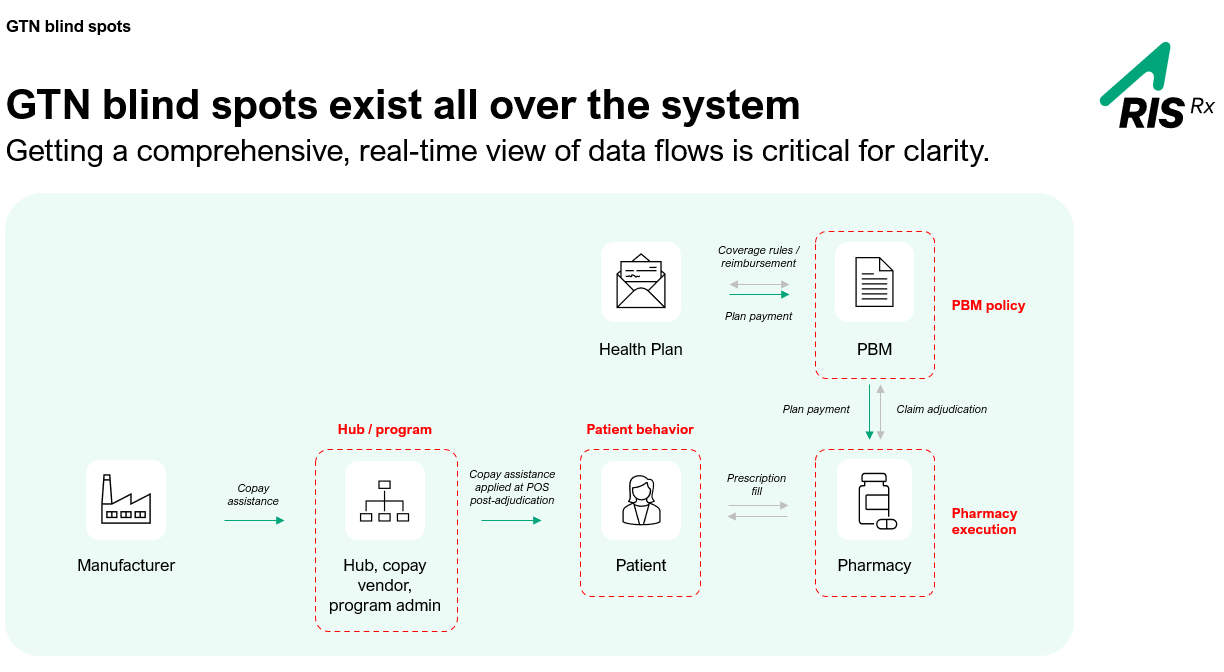
3. GTN Blind Spots Are Structural — Not Accidental
Here’s a question I asked during the webinar that I’d encourage every manufacturer to sit with: Where are your GTN blind spots?
The honest answer is: everywhere. Manufacturers fund the copay, but PBMs and pharmacies control where the dollars actually go. No single stakeholder in the chain — patient, pharmacy, PBM, health plan, hub, or copay vendor — sees the full picture. They all have partial data, different incentives, and different timing.
What makes this especially dangerous is that copay assistance is applied at the point of sale, after adjudication rules are already in place. By the time accumulator or maximizer logic kicks in, the damage is already being done. What we call “data asymmetry” is the core structural issue — and it’s why manufacturers keep feeling like they’re spending more while seeing less.
Bottom line: if your current visibility into the system starts at the second or third fill, you’re already too late.
4. Finance and Patient Services Are Looking in Opposite Directions
This was the quote I kept coming back to throughout the webinar — one I believe captures the organizational problem as well as any data point:
“When finance teams are looking backwards, and patient services teams are looking forward, leakage lives in the gap between them.”
GTN used to be treated as a backend financial reconciliation exercise. That made sense when the environment was simpler. But today — with maximizers growing more sophisticated, accumulators evolving around state bans, and specialty tiers expanding across more therapeutic categories — that organizational split is leaving real money on the table.
The manufacturers who are getting this right are fundamentally restructuring how finance and market access collaborate in real time, so the signal and the response happen at the same moment.
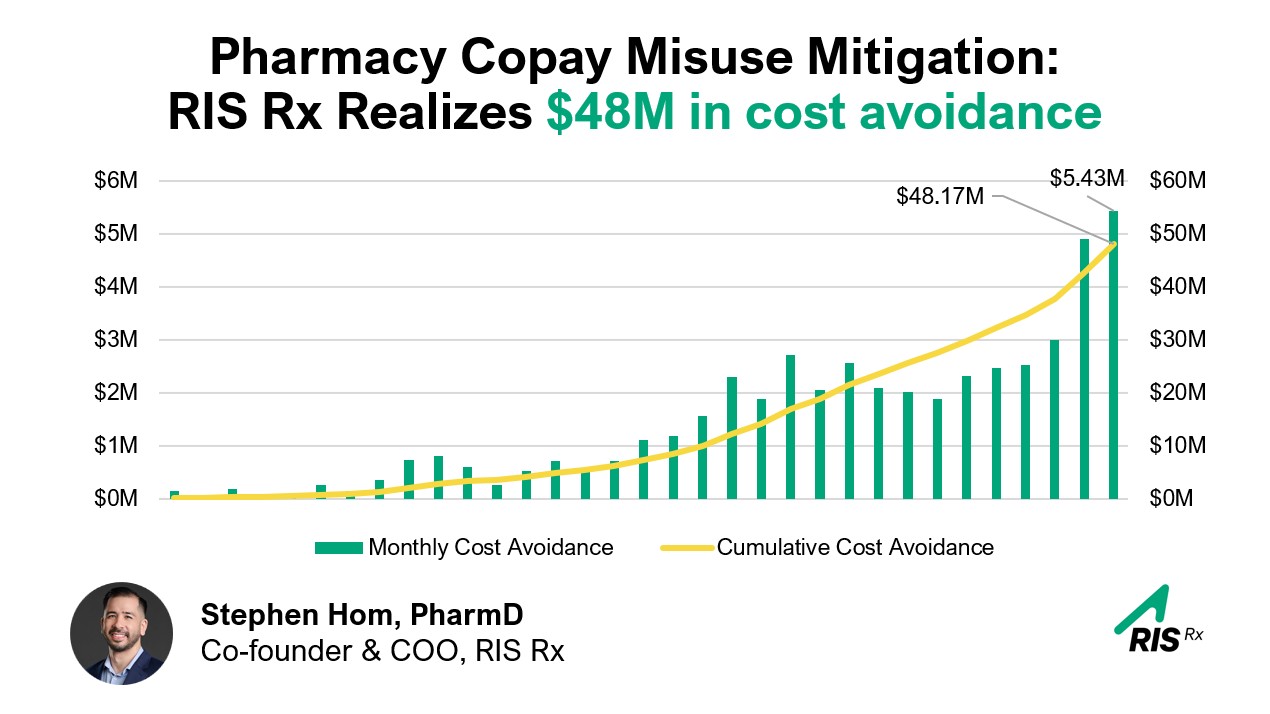
5. Real-Time Intervention Changes the Math — Fast
We shared several case studies in the webinar that I’m proud of, because they represent what’s actually possible when you move from retroactive reporting to proactive, enrollment-first intervention.
The through-line across all of the case studies is the same: timing is everything. Identifying leakage at enrollment, before first fill, is categorically different from identifying it at the second or third fill. Not just financially — but clinically and operationally too.
When you get enrollment right, spend drops, call volumes drop, patient out-of-pocket drops, and therapy starts faster. Those outcomes aren’t in tension with each other. They’re connected.
Want to Go Deeper? We’d Love to See You at Asembia.
If any of this resonates — and especially if you’re unsure where your own program stands — we’d love to talk.
We’ll be at Asembia 2026 (April 27–30), and we’re offering private, customized GTN exposure analyses for drug brands during the conference. This isn’t a sales pitch — it’s a working session where we look at your specific program, your channel, your benefit design exposure, and what the data actually says. Spots are limited, so if you want time with us in Vegas, reserve your meeting now.
The $90 billion problem isn’t going to fix itself. But it’s more solvable than most manufacturers realize — if you know where to look.